Dave Brown is a CEO / Founder of QiiQ Healthcare which is developing an AI assistant for healthcare workers, to invigorate the deep sense of fulfillment in delivering high quality care – frictionlessly.
In this episode, Dave shares how AI can improve healthcare by providing clinicians with actionable insights from patient data, making consultations more efficient. He highlights the challenge of adopting new technologies in healthcare due to risks and the complexity of changing established systems. Brown also shares insights on the economic impact of healthcare innovations and stresses the importance of doing thorough homework when entering the healthcare market.
Podcast: Play in new window | Download
Why you have to check out today’s podcast:
- Explore the impact of AI in healthcare and how it can improve healthcare outcomes and reduce doctor-patient interaction.
- Gain insights on healthcare pricing challenges and how understanding stakeholder decisions can lead to more effective solutions.
- Learn to navigate the massive, evolving healthcare industry and the challenges of making a meaningful impact through technology and pricing strategies.
“Do your homework. You cannot wander into this [healthcare] with youthful vigor and expect to change the world easily. And it’s certainly not easy to come up with a pricing model that everybody understands and likes.”
– Dave Brown
Topics Covered:
01:46 – How he got interested in pricing and why it mattered to him
03:13 – Detailing how QiiQ Healthcare technology works and what makes pricing for it complicated
10:58 – Sharing how QiiQ is driven by a social mission, as well as mentioning the real challenge in healthcare technology
13:49 – How QiiQ Healthcare technology is demonstrating its value in a leading Parkinson’s clinic
15:29 – Addressing patient willingness to pay and the impact of chronic diseases on society
18:34 – How QiiQ technology streamline doctor-patient interactions and save time
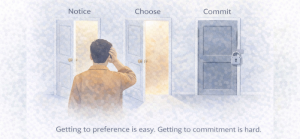
21:06 – Using the trolley problem to illustrate the complexity of decision-making in change management
23:31 – Highlighting the challenge of adopting new technology despite its potential, due to uncertainty and mental workload
25:34 – Discussing the challenges of accepting AI in healthcare, drawing analogies to self-driving cars and the risks involved
28:40 – Explaining how the relationship between cost reduction and profits in healthcare is complex and not solely driven by cynicism
29:45 – Dave’s best pricing advice
Key Takeaways:
“Everybody that’s working with me is driven by a social need or a social urge. It’s extremely common in the healthcare industry. But part of what you’re hearing [challenges] is motivated by a deeper grasp of the challenge in adoption. Without adoption, you generate no value.” – Dave Brown
Connect with Dave Brown:
- Website: https://www.qiiq.health/
- LinkedIn: https://www.linkedin.com/in/davecbrown/
Connect with Mark Stiving:
- LinkedIn: https://www.linkedin.com/in/stiving/
- Email: [email protected]
Full Interview Transcript
(Note: This transcript was created with an AI transcription service. Please forgive any transcription or grammatical errors. We probably sounded better in real life.)
Dave Brown
Do your homework. You cannot wander into this [healthcare] with youthful vigor and expect to change the world easily. And it’s certainly not easy to come up with a pricing model that everybody understands and likes.
[Intro / Ad]
Mark Stiving
Welcome to Impact Pricing, the podcast where we discuss pricing, value, and the vexing relationship between them. I’m Mark Stiving and I run boot camps to help companies get paid more. Our guest today is Dave Brown. Here are three things you want to know about Dave before we start. He’s the CEO and founder at QiiQ Healthcare. That’s spelled QIIQ. He’s been at that for eight years now. He was also the co-founder of Planet ECG. And by the way, he was in the audience of the webinar I did with Steven Forth and Michael Menzar put on by IbbaKa. and it was about Pricing of AI. Dave asked some really insightful questions and so I just invited him to join me here because he seemed like a smart guy. Welcome, Dave.
Dave Brown
I got you fooled.
Mark Stiving
Yeah, you did, Dave. It worked.
Dave Brown
It was actually an AI that asks all those questions, Mark
Mark Stiving
Was it? Okay? Got it. Well, I hope you’re typing your AI right now for the answers. So, well, I normally start out with the question, how did you get into pricing? I’m going to guess you’re not into pricing. How did you get interested or why do you think this is so crucial?
Dave Brown
Well, given the amount of time I’ve been working on this and I am, I would say an enthusiastic observer of what’s happening in industry. And I would say particularly the tech industry and modeling business for healthcare in particular, and just how difficult it is. And I’ve known Steven Forth as a friend for a long time, many years now, and I’ve also been a fan of his wisdom and acumen around pricing. I understand from observing him that he is a world leader in that domain. And it’s so tough in our business if you are going to provide technology to healthcare, you’re dealing with complexities that, well, if you’re selling pencils to consumers, you just don’t have any similar gauntlet to run. And sometimes I’m jealous of those simplicities.
Mark Stiving
I can imagine. So, before we hit record, you told me a little bit about what QiiQ does and some of the issues really fast. Tell us what QiiQ does, and then I’m going to explain why the pricing is so hard at QiiQ.
Dave Brown
Okay. So first, we are providing technology for clinical operations, at least for a portion thereof around data collection in the clinic, in order that the clinician can spend more time focusing on the patient and less time doing documentation oriented work. To simplify the architecture of that, the clinician is forced, has been for many years, forced to do the work of a data clerk or a scribe.
Mark Stiving
For those of us not in healthcare, can I just replace the word doctor with clinician?
Dave Brown
Clinician? Yep.
Mark Stiving
No, can I use the word doctor?
Dave Brown
You can, yes.
Mark Stiving
Okay, got it. Go ahead.
Dave Brown
…for the sake of this conversation. So the doctor spends a lot of their time doing low-skilled work in order that they can have an impact when they turn to working at ‘the top of their license’ which means doing the high skill work that they’ve trained so hard to do. So if we can use technology in most cases now, that’s AI that’s been appropriately tuned for the purpose. If we can use AI to offload that ‘low skilled work,’ the doctor’s time is much more high-skill-centric. That’s a goal to make good use, far more efficient use of the doctor and the nurse’s training in the exam room or around the patient at the clinic. They become a more profitable enterprise. Their capacity to take care of more patients rises and their ability to monetize value rises with that. Now, that’s part of it.
Mark Stiving
Let me just jump to the chase. You do this then by automating data collection at the patient. And so oftentimes it’s the patient using wearables or some other devices around their house. So we’re gathering data from the patient constantly on a regular basis so we don’t have to wait for the patient to come into the clinic.
Dave Brown
Well, yeah, but you’re sort of jumping to the other silo or the other domain of value creation here. I was talking merely about clinic operations, and you’ve raised the other, let’s say, quarter of the game. And that is the patient’s day-to-day life where so many relevant activities are happening. A night of four hours sleep or a week with no exercise. Or for some patients who require lots of medication that they skip dosages, or, are too late with them, and then they’re squeezing their dosages too close together. And that can be harmful, dangerous even, but it certainly is, let’s call it substandard from a clinical standpoint. So there’s a large amount of activity that has clinical relevance and today all of that great stuff and insight isn’t really getting to the physician, except when the patient can walk into the clinic and summarize it themselves by saying, ‘Yeah, lately, I haven’t been sleeping very well. And yes, I haven’t been taking my medications as per the prescription that you gave me last time.’ But most patients, when they’re in that very brief encounter with the provider, this stuff doesn’t come to them.
So if we can create a mechanism by which that patient’s 12 months of living and doing stuff that’s good or bad for their disease progression, well, if we can capture all that and summarize it in a way that the provider can use, boom. We’re generating significant value for both the patient and provider. And then there’s one more aspect of this that can really make a big difference, and that is if we’re able to intervene and support the patient day to day, week to week, month to month between their visits to the clinic, while we’re essentially running positive interference on behalf of the provider, making sure that the patient is taking their medication, is getting 6,000 steps in every day and sleeping a solid seven to eight hours, well, the provider’s going to love that because it makes their job easier, even while they’re not billing for that time, there’s value generated on behalf of the provider and the patient, of course feels better day to day, week to week, month to month. Yep. That’s a mouthful.
Mark Stiving
Okay, so now I want to share why, in my opinion, why this is such a hard pricing problem that you’re dealing with, right? It’s because you have three very different pricing problems all at once. So you’ve got the B2B pricing problem, meaning I’m going to help clinics be more effective. I could actually measure that in terms of patient output or how many doctor dollars I spend, right? So there’s a whole B2B conversation. There’s a B2C conversation. So can I get a consumer to buy an Apple watch or an Oura ring or whatever it is that we need them to be wearing? And then as you just expressed to me before we hit record, sometimes we get insurance companies involved, and now I’ve got to get insurance companies to figure out how much they’re willing to pay to help the consumer buy the product or pay the service. And so we’ve got three very different pricing problems and very different people or groups. So we’ve got to say, ‘Hey, you want to pay for this?’ We have to sell it to all three, which is now a real challenge for you.
Dave Brown
Huge. Yeah. So you’ve got three payers, patient, provider, and insurer, and who do you go to first? Who’s the first one to make the move? And how is value sustained over time? Like if you put yourself into the shoes of a patient. And maybe, Mark, you’ve had the displeasure of being one or parents that you’ve supported as they go through it. Who wants to interact with the clinic on a day-to-day basis? Like nobody. And so who’s going to, what patient is going to enthusiastically provide all this information in a well-formed summary to the clinic on a week to week, month to month basis? Well, no patient is going to do that actively with any gusto, so they need different incentives.
Mark Stiving
So I’m guessing that you went into this because you wanted to help people, help patients not necessarily to build a big business. And I say that because of the approach that I think you’ve taken.
Dave Brown
Well, without a doubt, everybody that’s working with me is driven by a social need or a social urge, right? To feel like the work you do is making the world better. Again, that’s pretty common to most people, I think. And certainly it’s extremely common in the healthcare industry, but part of what you’re hearing is motivated by a deeper grasp of the challenge in adoption. Without adoption, you generate no value. Lots of companies build technology for healthcare and they sell that technology into hospitals or clinics, but do doctors actively use it? Like I’ve talked to lots of doctors who hate the electronic health record system that they’re forced to use and they feel like it’s been imposed on them, and they will argue to the point of yelling that it generates no real value to them, but they have to use it because it’s required for them to do their jobs. But there’s a lot of other technology that isn’t required or obligatory, and they know it’s supposed to be useful, but damned if they’re going to figure out how to use that thing, so forget it. So, yes, a big sale worth a lot of money to both the clinic and the vendor who sold it, but little value where it really counts for the provider and delivering health support to their patients.
Mark Stiving
Yeah. Fascinating problem. So you just added a fourth layer and that fourth layer is how do I get doctors to actually choose to use this, right? How do I get doctors to buy into it? And so this is really challenging. As I listened to you talk, a solution came to my mind, and by the way, tell me that I’m totally messed up. It never bothers me to be wrong, but I could see how there’s a small market segment that isn’t what you’re after today that would really dive into this. And that is, let’s call it sports medicine, or let’s call it the people who want to pay money because they want to be really healthy. And so I would happily buy an Apple watch and an Oura ring and a sleep detector and anything you want me to buy and put in my house. And then I would have a doctor, I would pay a doctor to go watch that and say, ‘Hey, what’s going on day-by-day-by-day?’ And that might be an interesting way to get penetration, to get data that says, ‘Hey, look at how well this works,’ and people are buying into this concept. And the other nice thing is I don’t have to sell to insurance companies then, right? I’m just picking the cream of the crop at the beginning.
Dave Brown
It’s not far from what we’re doing. Like right now, we’re finishing delivering a portion of the whole network solution onto Parkinson’s disease clinics. Well, we’re building for one clinic in particular that’s especially world leading and progressive in terms of innovation. Now, Parkinson’s is not the same as sports injuries. But from a, let’s call it an information architecture point of view, it’s very similar. We expect to demonstrate proof of real value delivered, manifest not just in improved efficiency for the clinic, but also for an improved experience for the patient. And that will be an important, let’s say, tagline for sports clinics and other specialties that have the same information problem.
Mark Stiving
Yeah. So, the big difference I would see between Parkinson’s and sports medicine or health nuts, if you want to call them health nuts for the sake of argument, is that health nuts have this desire to pay for this. They’ve got a higher willingness to pay than a Parkinson’s patient. So I could see a Parkinson’s patient being the same as any other kind of patient that says, ‘Look, I’d like to be healthy, but I don’t want to buy all this stuff. I don’t want to do all this stuff, right? Can’t you just give me a pill and fix it?’ Where I think health nuts have a desire to pay money to know more.
Dave Brown
Well, I appreciate that distinction and I understand it because I’m a sportsman, I guess you could say elite or semi elite for a long time, and I understand that motive. I would not discount the ambitions of an informed Parkinson’s patient; most at some point become extremely informed on the challenge because it imposes on their life and moment to moment ways. You know, the tremors and the movement challenges are so vexing that their incentives burn at them all the time, more so than, and the most ambitious athletes who are training twice a day or three times a day. It creates desire. And that’s not something to exploit. It’s something to support and commit to to relieve suffering and profound life disruption, I mean, extremely motivating for us and for clinics.
Mark Stiving
Yep. And I don’t like the word exploit in that sense, because in truth, what we’re trying to do is get them to cover the costs, right? And so it doesn’t really mean, ‘Hey, we’re going to try to make a ton of money off of you. We’ll make that money off the clinic.’ It’s okay, right?
Dave Brown
Well, you might say, Mark, that there is a little bit of Amazonian thinking here. We minimize, or let’s say, we thoughtfully manage the cost to the patient in a controlled, let’s call it compassionate fashion. But at scale when you look at the massive array of chronic diseases: cancer, dementia, on top of things like Parkinson’s that affect a smaller portion of the population, there are two things that become obvious. One, there are a lot of people that need support and live with these challenges. Cancer in particular, right? It gets pretty much everybody, if they live long enough. and the cost to the general public, to the treasury, the federal treasury or provincial treasury is so massive. We’re looking at a significant fraction of, let’s call it the tax burden of regular folks. So it’s something that if impacted in a meaningful way has massive economic consequences for everyone.
Mark Stiving
So Dave, can you give us an example of how collecting data from my home reduces the cost or the amount of time a doctor has to spend with me? Because I would almost think it increases it because now there’s more information, there’s more tasks, more things to do.
Dave Brown
Great question. Thanks for that one. It almost sounds like a low ball by design. So if you have a chronic condition, you go into the clinic, you may have 45 minutes with your doctor, a neurologist in the case of Parkinson’s, or, an oncologist in the case of cancer and a big chunk of the time that they spend with you, they’re asking a pile of routine questions. Tell me about your life. How are things going? How’s your sleep been? How’s your relationship with your children? Have you continued having the conflict at home that you were having, you told me about last time? And how’s it affecting your sleep. A ton of time, sometimes half or more is spent on interviews that consume or cover that ground. And if we can displace that time or port it, transpose it over to, let’s say an automated function that happens over months, well all those answers become available within a larger corpus of data.
And then the challenge and the task for a well-trained AI is to shrink it down and turn it into a summary with valid actionable insight for the provider that they can consume in 30 seconds to 90 seconds prior to walking into the exam room. So the moment they step into the exam room, they know all this stuff, or at least the parts that matter so that they can jump right into, ‘Wow, Mark, I understand what you’ve been going through now I see that your sleep has been in decline, and clearly your anxiety levels are on the rise. Let’s do something about that.’ And every patient wants that kind of value.
Mark Stiving
Yeah. So, when I asked you what we were going to talk about today, you had said how to make this work in a market that hates change and risk. So do you really think they hate change, or do you think it’s just that change is hard and you have to change the behavior of consumers, of clinicians, of insurance companies? It’s like a really large change management problem.
Dave Brown
Yeah. It’s not an easy one, but I often refer to the trolley problem. Are you familiar with that one, Mark?
Mark Stiving
Go ahead and share with all of us.
Dave Brown
You are a railroad conductor standing beside a railroad track. And in front of you is a lever that would switch the rail line from one track to another track. To your left in the distance is a train hurtling towards you and this branching exchange at a blazing rate. And on the default track stands a group of people 50 in number who as you’re standing there in front of that lever, they will be obliterated by this train. If you throw that lever, you switch off the default track to a secondary track, but you cannot see who’s on that secondary track. But you have a sneaking suspicion that there’s a gorgeous lovable 18-year-old valedictorian standing on that track. You don’t know for sure, but she or he might be there. And if you throw that switch, that death is accountable to your decision to throw the switch. It’s your fault she died. Now, you will be saving 50 people, and they’ll never know it because they don’t know that they were about to be obliterated, or they just assumed that that was going to happen anyways. And they don’t know that you had anything to do with changing their fate. You are only accountable for the damage you’ve done to the unfortunate on the secondary track. And that’s why it’s a great story. That’s why no executive wants to throw the switch.
Mark Stiving
So, I don’t get it though because for me to adopt your technology, I don’t have to change what I do today. I can just use it as, ‘Hey, I’ve got additional information. Do I want to use this information or not?’ So it isn’t like I’m forcing you to go kill ‘ else. I’m just saying, ‘Hey, look, there’s more info. Do with it what you want.’
Dave Brown
Well, yes and no. We are talking about technologies that aren’t perfect, and AI, as most of us now know, isn’t perfect, right? It has a tendency to hallucinate. So that’s one thing that introduces uncertainty into the picture and makes you a bit blind to what’s waiting for the train on the secondary track. The evil you know is better than the evil you don’t know. So that’s one factor. And it’s an easy out, ‘Hey, if your technology isn’t proven to be flawless and perfect, well it’s easier for me to just stand back and avoid throwing that lever.’ Now, in throwing the lever in my analog, the trolley analog. It’s a very easy action, but deploying technology into a clinic and adopting its use even when it’s well designed, and that’s a central objective we have, it’s still work. It’s cognitive load to think differently about the thing that you’ve been doing for some 20 years. Eh, I know it’s going to be better, but it’s just different. And I don’t have time to think about that. I’m just going to keep operating the same way I always have. And I’m speaking as a theoretical doctor who is just racing to retirement and doesn’t want to flip any switches.
Mark Stiving
That’s exactly how I was thinking about AI until Steven Forth, just like, beat me into spending time with it.
Dave Brown
Wait, did you think it was perfect and Steven convinced you that it was not or the other way?
Mark Stiving
No. I thought it was additional work, something I didn’t have to learn and use because I know what I’m doing. Leave me alone. Right? But I’ve seen studies now that show, and I’m shocked that every clinic doesn’t know this or believe this. Studies that show doctors using AI have much better outcomes than doctors alone or AI alone.
Dave Brown
Yeah, I mean, it takes time, Mark, for a revolution. Like we’re observing now to take real root in, let’s call it in the zone of maximal impact. Healthcare, if something goes wrong, people can die because of it, and it just creates more weight and more inertia for the status quo.
Mark Stiving
So, let me draw another analogy.
Dave Brown
Go ahead.
Mark Stiving
The analogy of self-driving cars. Turns out self-driving cars are way, way, way safer than people driving cars, but as soon as someone dies in a self-driving car, someone gets sued, right?
Dave Brown
I love that analog, even though it’s so depressing. It really does underscore… So what would you account that for, Mark? Why the lack of thoughtful reason?
Mark Stiving
I think it’s pretty simple. It’s the fact that I have accepted certain risks, so I’ve accepted the risk that other people are driving and people make mistakes, but I haven’t accepted the risk that Elon Musk is allowed to kill me if he makes a mistake.
Dave Brown
That’s well said. Yeah. So that’s a trolley problem, but sort of amplified in the public sphere.
Mark Stiving
And that’s why I also love the studies that say AI with doctors have the best outcomes, right? It’s kind of like saying, I want an automatic, I want an EV that drives autonomously with someone sitting behind the steering wheel.
Dave Brown
So if I wasn’t excited about the same thing those studies and more and if I wasn’t so aware of the cost of doing nothing the default track, so to speak. And that cost, Mark, is massive at scale, and it’s soul crushing to really contemplate its proportions and how much we all pay for it. So yeah, we’re motivated knowing that when fully realized AI’s impact on healthcare will provide relief to all of us in ways that I know very few of us can imagine at this point.
Mark Stiving
And I’m going to make one last pricing comment about this whole thing, and I could be so far off base because I don’t spend too much time in pricing healthcare, and that is, it seems to me that healthcare companies do their best to not reduce costs because it means it also reduces their profits. And so that may be a driving factor to what it is that you’re facing.
Dave Brown
Yes and no. It depends on what slice of the cost pie we’re looking at and who’s participating in who the stakeholders are and the value delivery and realization. Yeah, I don’t need to tell you that it’s a cynical view, and it is true in some cases, but in many cases, that’s not really what’s behind the rather cynical decisions that we see being made all the time. But let’s talk about pricing some more. I mean, I’m happy to get into that a little bit.
Mark Stiving
I’d be happy to, but we’re out of time. Oh, I’m going to wrap up the podcast and then I’d be happy to talk to you more afterwards if you’d like.
Dave Brown
Well, we’ll take a couple minutes for it. I’ve got a nasty task list for the day, but sure.
Mark Stiving
Okay. So Dave, as we wrap this up, I do want to ask you the final question. If you can even come up with an answer to this one. What is one piece of pricing advice you would give our listeners that you think could have a big impact on their business?
Dave Brown
Well, broadly speaking, I don’t know that I have any useful guidance that outstrips what you can toss off in a second. But I will say to the many who are seriously considering tackling the healthcare problem, because the, let’s say the whole nut is so massive, do your homework. You cannot wander into this with a youthful vigor and expect to change the world easily. There is a lot of money moving into, through and out of healthcare, but it’s not easy to grab a piece of that. And it’s certainly not easy to come up with a pricing model that everybody understands and likes.
Mark Stiving
Nice. It sounds like it’s way more than finding a place where you can add value. It’s really understanding all these different decisions that are being made and how are you going to get people to change the way they make decisions.
Dave Brown
Yeah.
Mark Stiving
Excellent. Dave, thank you so much for your time today. If anybody wants to reach out to you, how can they do that?
Dave Brown
Well, I’m easily found, anybody can find us easily on our website. It’s QiiQ.health, that is Q-I-I-Q, health, H-E-A-L-T-H. Oh, and I’m on LinkedIn. If somebody looks for me on LinkedIn, Dave Brown, well, there are a lot of Dave Browns, but I’m in Vancouver, British Columbia, and my avatar is a blue head.
Mark Stiving
I was going to say, you look like one of the blue man groups.
Dave Brown
Yeah, I get that a lot. And it was by design.
Mark Stiving
Nice. To our listeners, thank you so much for your time. If you enjoyed this, would you please leave us a rating and a review? Tammy T left me a nice Amazon review for the book, Selling Value. She said:
“The emphasis on understanding and delivering real value shifted how I approach sales. It’s less about persuasion and more about building trust, making the entire process feel authentic and rewarding.”
Tammy, that’s beautifully said, and the check is in the mail. Finally, if you have any questions or comments about the podcast or if your company needs help getting paid for the true value, feel free to email me, [email protected]. Now, go make an impact!
[Ad / Outro]